Pediatric CNS Examination
The paediatric central nervous system (CNS) examination is a key component of the emergency department assessment. It systematically evaluates mental status, cranial nerves, motor and sensory systems, reflexes and developmental milestones, helping to identify time-critical pathology (raised ICP, meningitis, encephalitis, status epilepticus, spinal cord lesions) and guide further investigation.
Mental Status Examination
The mental status exam in children focuses on level of consciousness, behaviour and age-appropriate cognitive function rather than formal “mini-mental state” testing.
- Appearance & behaviour: posture, movements, agitation vs lethargy, eye contact, interaction with caregiver.
- Level of consciousness: alert, responds to voice, responds to pain, unresponsive (AVPU or paediatric GCS).
- Speech & language: age-appropriate vocabulary, fluency, articulation, following simple/complex commands.
- Mood & affect: appropriate to situation, irritable, withdrawn, inconsolable, labile.
- Thought content & perception (older children): confusion, hallucinations, delusions if suspected.
- Memory & orientation (age-adapted): name, parents, place, recent events in older children.
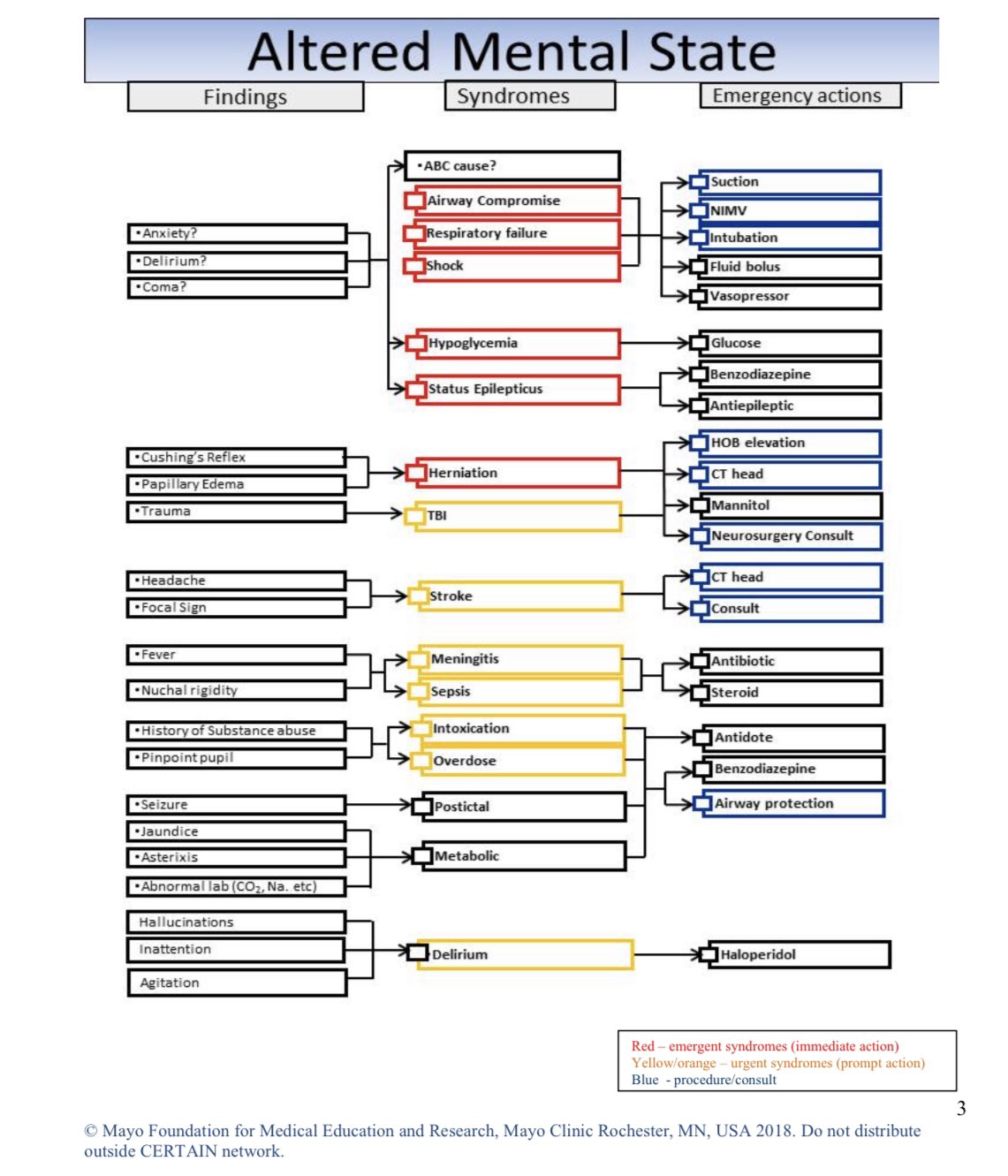
Altered Mental Status – Visual Aids
Click images to enlarge.
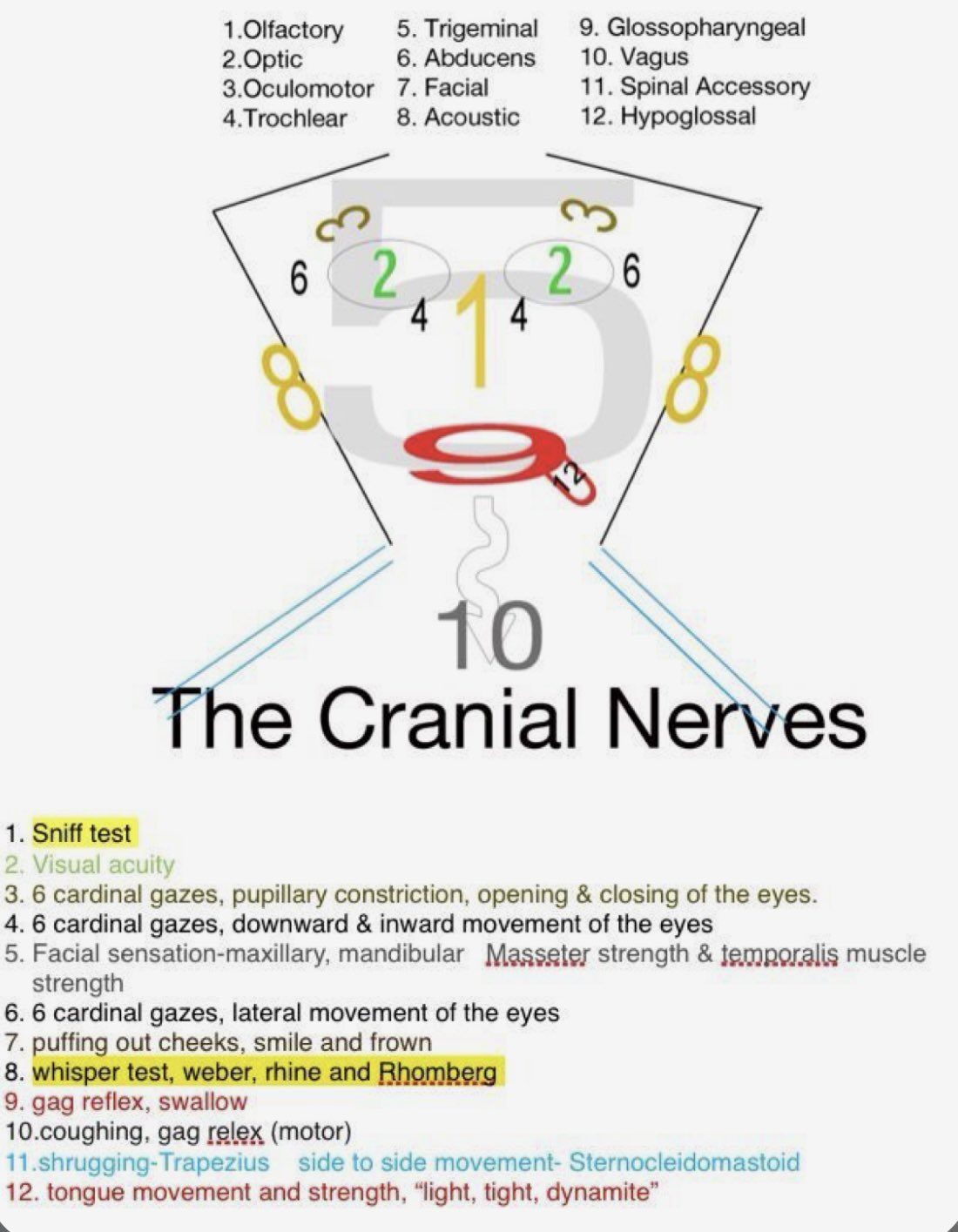
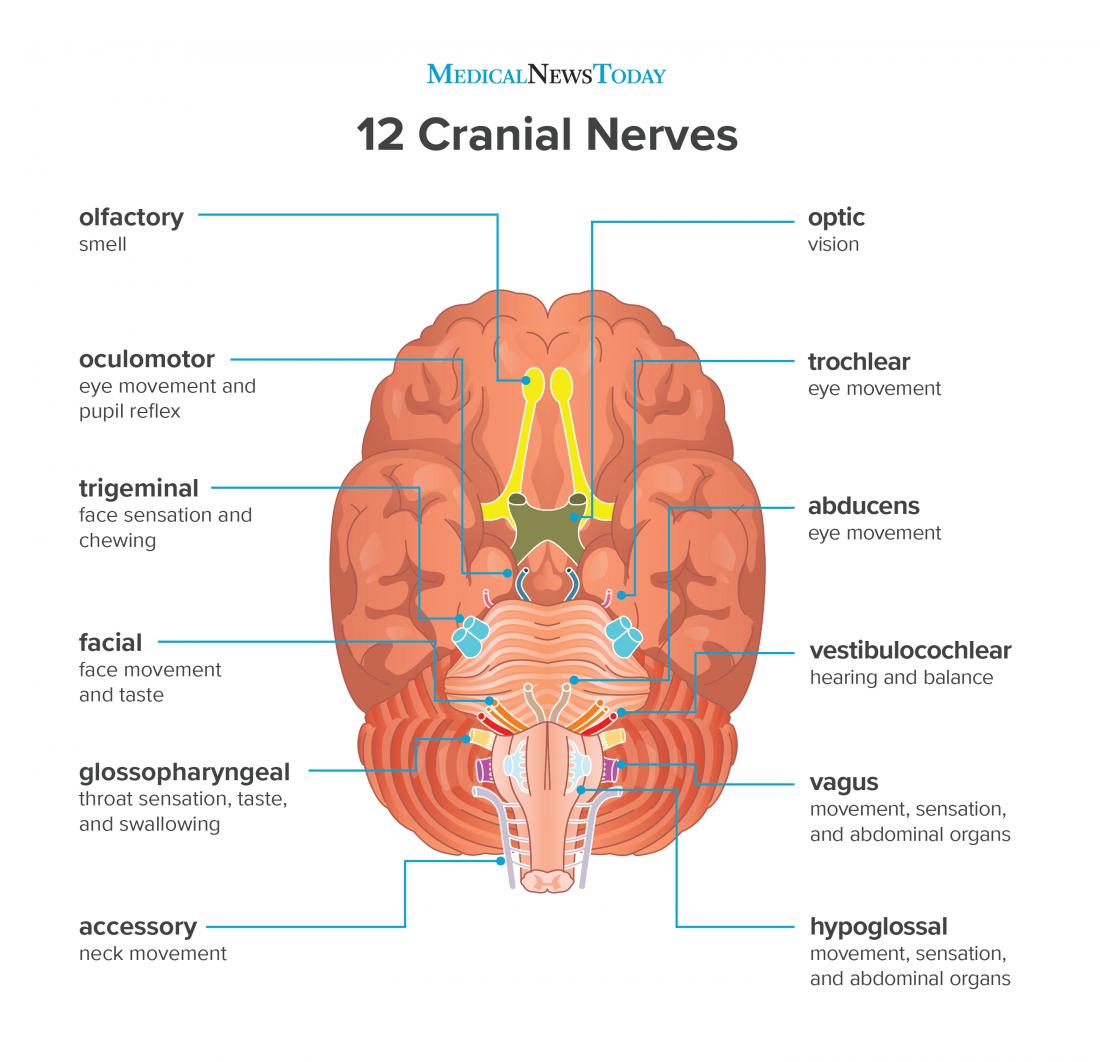
Cranial Nerves Examination
Cranial nerve testing in children must be adapted to age and cooperation level. Use toys, lights and games.
- I – Olfactory: usually omitted in the ED; can test with familiar scents in older children if needed.
- II – Optic: visual behaviour in infants, fixing and following; older children – visual acuity, visual fields, fundi.
- III, IV, VI – Oculomotor/Trochlear/Abducens: eyelid position, pupil size/reactivity, full range of eye movements; note nystagmus or diplopia.
- V – Trigeminal: facial sensation (light touch), jaw opening/closing; corneal reflex if indicated.
- VII – Facial: eye closure, smile, show teeth, puff cheeks; look for asymmetry or droop.
- VIII – Vestibulocochlear: response to sound in infants; whisper tests or tuning fork in older children; balance if walking.
- IX, X – Glossopharyngeal/Vagus: voice quality, swallow, palate elevation, gag (if needed); cough strength.
- XI – Accessory: shoulder shrug and head rotation against resistance.
- XII – Hypoglossal: tongue protrusion and movement; look for deviation, fasciculations or wasting.
Motor System Examination
Assess bulk, tone, power and coordination, comparing sides throughout.
- Muscle bulk: look for wasting, asymmetry, pseudohypertrophy.
- Tone: passive movement in limbs – hypotonia vs spasticity vs rigidity; note head lag in infants.
- Power: age-appropriate tasks (pushing/pulling, standing from squat, climbing onto bed, lifting limbs against resistance).
- Gait & balance: normal gait, toe/heel walking, tandem gait in older children; sitting/standing transitions in toddlers.
- Coordination: finger-nose, heel-shin in older children; reaching for toys in younger children.
Sensory System Examination
Sensory testing in young children is often limited; focus on symmetry and gross deficits rather than detailed dermatomal mapping in the ED.
- Light touch and pinprick: compare both sides of face, upper and lower limbs.
- Temperature: cold metal or cool/warm object if needed.
- Vibration: tuning fork over bony prominences (malleolus, wrist, sternum) in cooperative children.
- Proprioception: up/down movements of fingers or toes, asking child to report direction.
- Cortical sensations (older children): two-point discrimination, stereognosis, graphesthesia if clinically indicated.
Reflexes Examination
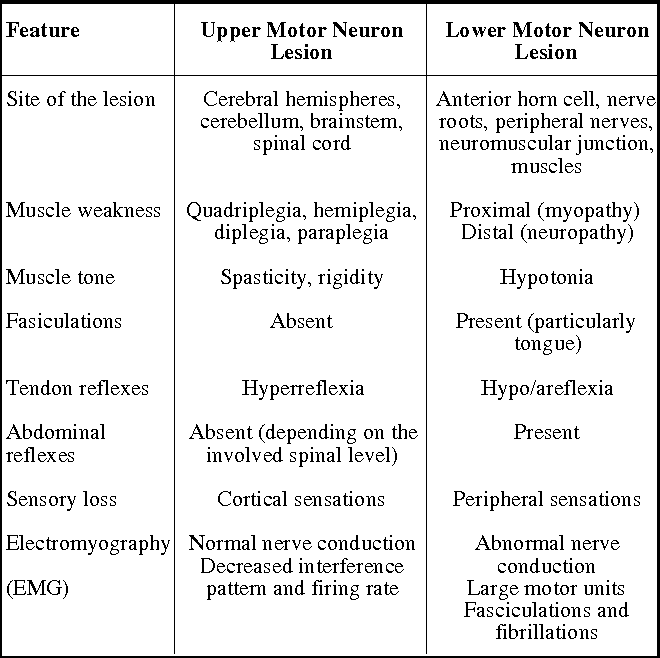
Deep tendon reflexes help distinguish upper vs lower motor neuron lesions.
- Deep tendon reflexes: biceps, triceps, supinator, patellar, Achilles; grade 0–4+ and compare sides.
- Plantar response: flexor in older children; an extensor (Babinski) is normal up to ~1 year but abnormal thereafter.
- Clonus: sustained ankle clonus suggests upper motor neuron pathology.

Neonatal Primitive Reflexes
Primitive reflexes are key indicators of brainstem and spinal cord integrity in newborns and young infants. They should appear and disappear at expected ages.
- Moro (startle) reflex: extension then flexion of arms with startle; present at birth, usually gone by 4–6 months.
- Babinski reflex: toe fanning with stroking of sole – normal in infants, should disappear as corticospinal tract matures.
- Rooting reflex: head turns toward stimulation at cheek/mouth; helps with breastfeeding.
- Palmar/plantar grasp: strong grasp of object placed in palm/sole.
- Asymmetrical tonic neck reflex (ATNR): “fencer” posture when head turned; should fade by around 6 months.
Persistence of primitive reflexes beyond expected ages, or asymmetry, can indicate CNS pathology and should prompt further evaluation.
Developmental Milestones
Comparing CNS findings with developmental milestones is essential. Delays in one or more domains (gross motor, fine motor, language, cognitive, social) may be the first clue to neurological disease.
| Age | Gross Motor | Fine Motor | Speech & Language | Cognitive | Social & Emotional |
|---|---|---|---|---|---|
| 0–3 months | Lifts head briefly when prone | Grasps objects reflexively | Cooing, gurgling | Follows objects with eyes | Responsive to familiar faces |
| 4–6 months | Rolls over both ways | Reaches for and holds objects | Babbling with consonants | Explores objects with hands/mouth | Laughs, shows excitement |
| 7–9 months | Sits without support | Transfers objects between hands | Varied babble with inflection | Bangs objects together | Stranger anxiety, shows affection |
| 10–12 months | Crawls, pulls to stand | Pincer grasp, feeds self | First words, gestures | Simple problem solving | Imitates actions, waves goodbye |
| 13–18 months | Walks alone, climbs stairs with help | Builds tower, scribbles | 5–10 words, follows simple commands | Matches objects, simple sorting | Shows affection, imitates play |
| 19–24 months | Runs, kicks ball | Turns pages, uses utensils | 2–3 word phrases, names objects | Understands simple routines | Parallel play, emerging defiance |
| 2–3 years | Jumps with both feet | Strings beads, begins scissors | Short sentences, names self | Sorts by shape/colour, counts to 3 | Plays near others, empathy emerging |
| 3–4 years | Hops on one foot | Draws basic shapes, buttons | Asks many questions, retells stories | Matches, sorts, counts to 10 | Cooperative play, shares toys |
| 4–5 years | Skips, throws/catches ball | Prints letters, more complex drawings | Clear speech, detailed stories | Names colours, counts to 20 | Group play, sense of humour |
| 5–6 years | Balances on one foot, rides bike | Writes name, ties laces | Complex sentences, retells events | Understands time, counts higher | Stable friendships, rules in games |
Common Pediatric Neurological Conditions
CNS examination findings and milestone review help screen for a range of paediatric neurological and neurodevelopmental conditions:
- Cerebral palsy: non-progressive motor impairment, abnormal tone and posture, delayed milestones.
- Global developmental delay / intellectual disability: delays across multiple domains; often first recognised via milestone surveillance.
- Neuromuscular disorders: e.g. muscular dystrophies, spinal muscular atrophy – proximal weakness, Gowers sign, reduced/absent reflexes.
- Epilepsy: recurrent unprovoked seizures; may have focal deficits or regression if poorly controlled.
- Autism spectrum disorder (ASD): social communication difficulties, restricted/repetitive behaviours, sensory differences.
- ADHD: inattention, hyperactivity, impulsivity affecting school and home functioning.
- Childhood migraine and headache syndromes: recurrent headaches ± vomiting, photophobia, triggers.
- Acute CNS infections/inflammation: meningitis, encephalitis, ADEM – fever, headache, photophobia, seizures, focal deficits or altered behaviour.
Conclusion
The paediatric CNS examination in the ED should be structured but pragmatic, adapted to the child’s age and condition. By systematically assessing mental status, cranial nerves, motor and sensory systems, reflexes and development, clinicians can promptly recognise serious pathology, initiate urgent treatment, and arrange appropriate imaging and specialist referral.